
Top 10 Things to Keep Air Clean In A Dental Office: Capturing Aerosols and Splatter
Read More
COVID-19 INFO
Dear Tooth & Co Families and Patients,
As the facts and situation around COVID-19 (coronavirus) continue to evolve, and in step with Governor Tim Walz’s recent Declaration of a State of Emergency, the Minnesota Dental Association (MDA) and the Minnesota Board of Dentistry made their recommendation on Monday, March 16th, that dentists practicing in Minnesota voluntarily suspend nonessential, or elective dental care for the next 14 days. As always, it is expected that dentists continue to be available as needed for emergency care and services and we want you to know that we are here for you at Tooth & Co. If your child experiences any discomfort related to their mouth, be it due to caries, trauma or else, don’t hesitate to call the office number. We will triage and treat accordingly. Tooth & Co is your dental home.
This temporary change is done out of an abundance of caution during this historic public health emergency. As health care professionals, we all have a role to play in "flattening the curve" in order to follow sound, scientific public health advice to help limit infections and slow the spread of the virus. The best resource for up-to-date information on COVID-19 is the Centers for Disease Control & Prevention (CDC) website. https://www.cdc.gov/coronavirus/2019-ncov/index.html The CDC website is updated daily and contains truthful, scientific information that individuals and families can trust.
Until further notice we will implement a few changes in the clinic in order to reduce the potential spread of infection.
· We have removed the toys, stuffed animals, books, magazines, and stickers/treats.
· We thoroughly and frequently clean items that can be cleaned in the common areas, including furniture.
· To reduce exposure, we ask that you wait in your car until your appointed time.
· We ask that you sanitize hands upon entry. Hand sanitizer will be provided.
· We require that you limit family members attending visits in order to minimize hand contact and unnecessary touching.
What we will not change is our customary and very strict daily infection control protocols and procedures which keep our patients and staff safe from the spread of illness and disease. We hope to reopen with a regular schedule as early as Monday, March 30th, but will monitor this ever-changing situation and continue to adhere to the latest recommendations by the state. One of our staff members will be contacting you in the coming days in order to reschedule your appointments. Please call if you have any questions or emergencies and we will assist you as promptly as possible. We want to thank you for your understanding during this time and wish you and your families the best.
Dr. Ellie Sakhi
**BACK TO SCHOOL**

With summer quickly coming to an end, it’s time to start thinking about a healthy back to school routine. Did you know that tooth decay is still the most common chronic disease in children, 5 times more common than asthma? Cavities can cause problems with your child’s daily activities, such as sleeping, eating and learning, which can lead to a not fun school year and missed school hours. Start your child’s school year off right with these helpful tips.
1. Routine dental visits every 6 months
Set up your child’s next dental check-up at Tooth & Co Pediatric Dentistry. A check-up will ensure a healthy start to the school year.
2. Establish Healthy Habits
Have your child brush teeth before leaving the house in the morning. Most school mornings have little time to spare. Keep morning brushing as one of your “can’t miss” steps before heading out. They’ll start the day with fresh breath and a bright smile.
3. Don’t eat after brushing teeth
This is especially important before bedtime, as salivary flow decreases while they sleep, and teeth become more vulnerable to cavities.
4. Eat Nutritious Foods
Encourage healthy eating. Tooth friendly snacks include fruit, cheese, vegetables, and nuts. Avoid sticky foods, such as candy, fruit roll ups, and granola bars. These foods stick to teeth surfaces and cause decay.
5. Don’t nibble food or sip continuously
Allowing time between snacking and sipping allows saliva to neutralize acids and repair teeth.
6. Choose Water
Juice and soda often contain more sugar than children should have in an entire day. This sugar can coat the teeth, promoting tooth decay. Too much sugar may also lead to an afternoon crash, which in turn interferes with schoolwork. Instead, give your kids fruit and frequently remind them to drink water.
7. Be safe
With back to school comes school sports. Make sure kids participating in organized sporting events wear mouth protection. Kids should also remember to wear a helmet when riding bicycles, scooters, and rollerblading.
8. Ask About Sealants
Dental sealants can also protect your children’s teeth from cavities. Sealants, which are applied to the chewing surfaces of molars, act as a shield between the tooth and harmful bacteria.
Finally, it’s recommended to bring your kids in every six months for an exam, cleaning and fluoride treatment. If you haven’t made an appointment, give us a call, email or send an appointment request and we will happily get you on the schedule.
We hope your school year starts out all smiles.

Tooth & Co Pediatric Dentistry
Nurturing Young Smiles

Summer is not over!
Summer is not over, but it sure is going by fast!! Be sure to call us to schedule your child's dental visit while there may be spots left. We want to make sure all of our patients get to start a new school year with healthy, and squeaky clean teeth :) Call/email/PM tooth & co pediatric dentistry. Our specialty:
NURTURING YOUNG SMILES
#pediatricdentistry #healthyteeth #backtoschool #childrensdentisty
Gift some good, clean fun with Tooth & Co!



Looking for holiday gift ideas? stocking stuffers?
Look no further - we’re excited to announce that we now carry Sonicare brushes and an in-home whitening product for the entire family!
Sonicare Kids brushes are a great way to get kids excited about brushing and healthy habits with its Bluetooth compatibility and fun teaching app. When you purchase your Sonicare Kids toothbrush from our office, they’re just $34.99 after $5 mailed rebate with an additional brush head and extra 6 months of warranty.
For our older patients (and parents!), we now carry the Sonicare Flexcare Platinum Connected toothbrush. We’re excited to introduce this Bluetooth-connected super-brush at an awesome Holiday Special price of $99.99 after $20 mail-in rebate ($60 off suggested retail pricing!). If purchased through our office you’ll also enjoy an additional six months warranty (2.5 years total), 3 versatile bonus brush heads (total of 4) and a deluxe traveling case, perfect for holiday journeys.
We’d also like to share that we now carry Philips ZOOM Whitening pens - a great way to keep your teeth merry & bright while on the go. Each pen contains approximately thirty full applications of easy-to-apply whitening gel, approximately a 2-week supply with directed use. These pens are $19.99 and only available through your dental professional. These pens are safe, do not cause sensitivity, and have a very mild mint odor and taste. Philips recommends this product for ages 13 and up.

Here Comes the Sun!
Summer is fast approaching and with it plenty of fun. Changes to your school-year routine can be a welcome change of pace, but it’s important that one routine stays consistent – your dental hygiene. Here are a few ways to have plenty of summer fun while keeping your oral health in top shape:
Camps, Vacations, and Sleepovers

Overnight trips can be an exciting change of scenery for kids, but it’s important to keep up your usual morning and night dental care routines!
Remind children before they leave for a sleepover to brush before bedtime and after breakfast!
Be sure that toothbrushes, toothpaste, and floss are packed before leaving for vacation.
Having a new character toothbrush or a fun travel-size toothpaste saved specifically for overnight trips is a great way to get children excited about brushing away from home.
Outdoor Activities and Summer Sports
Summer is made for spending time in the great outdoors, and no matter your family’s activity of choice, it’s important to put safety first!
Bicycles, skateboards, and roller skates should be accompanied by a well-fitting helmet.
A mouth guard is a great way to prevent dental injuries during contact sports.
In case of any dental injuries, call Tooth & Co right away!
Sunscreen and plenty of water should be available at all times while playing in the sun!
Sips, Snacks, and Sweets

From Fourth of July parties to the neighborhood ice cream truck, summer can be full of opportunities for sugary snacks and drinks.
Bringing tooth-friendly options (like fresh fruit, cheese sticks, or veggies and dip) to your summer get-togethers can ensure there’s always something healthy to choose!
A less-structured day may increase your child’s requests for snacks, but it’s important to maintain a regular meal schedule with only a few snacks in between.
Snacking often between meals means teeth are repeatedly exposed to food. If food is left for a long time, your child may be at higher risk for decay.
Snacks high in protein like nuts, hummus, or Greek yogurt (watch for added sugars!) can help keep your family full between meals.
Hydration during the summer months is of utmost importance, but what your child sips on is as important as how often.
Water is the ideal choice for hydration! Juice and sports drinks are best left for special occasions.

Have a healthy, happy summer!
- Dr. Ellie & the Tooth & Co Team

It’s Back-to-School time!
Back To School!
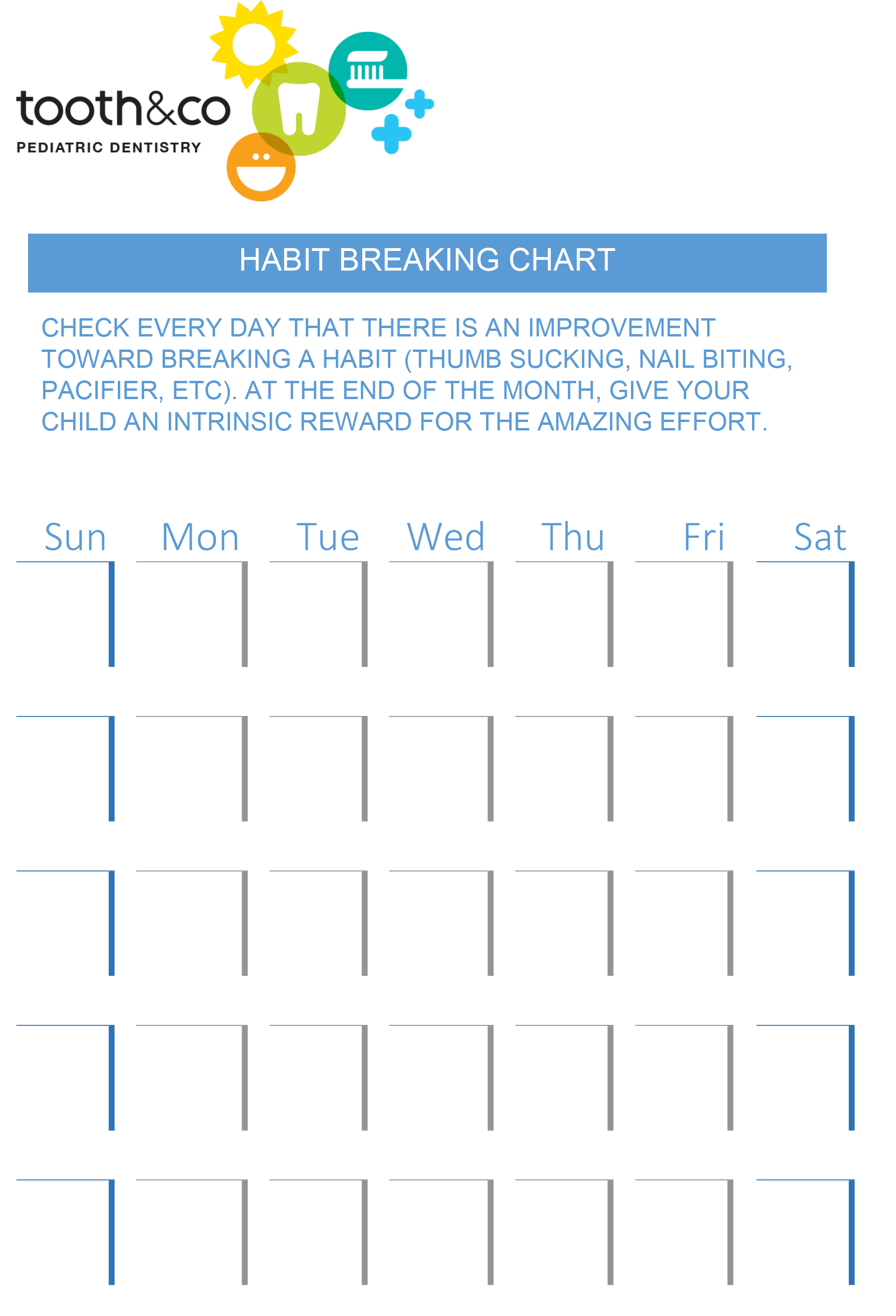
Read MoreHabit Breaking Chart for Home
Filling in a daily chart may be just what your child needs to set small goals and work toward the ultimate goal of breaking a habit. Print out the chart, and have fun filling in or gluing an icon (see below) in the appropriate day of the week. Be sure to let us know how this works out for you.

Tooth Brushing & Flossing Chart for Home
Here is a chart to help motivate kids and parents towards a sound daily routine. It is up to you how you would like to reward your child for working hard and doing a great job. We recommend parents to assist children with both brushing and flossing until they master the techniques and effectively remove plaque from all surfaces of their teeth. Please let us know if you have any questions or comments regarding your child's home care. Our assistants are specially trained to give oral hygiene instructions to children of all ages, and give parents tips to make home care easier and more pleasant for everybody.

FLUORIDE; Topical versus Systemic
WHAT IS FLUORIDE?
Fluoride is a mineral that is found naturally in soil, water, and foods. It's concentration in seawater is about 1.3 ppm (parts per million), and typically in freshwater ranges from 0.01 to 0.3 ppm. Outside of the United States in some area of the world, naturally occurring fluoride is much higher. Fluoride can also be made in laboratories, which is then commonly added to drinking water, toothpaste, and other various products.
WHY IS FLUORIDE ADDED TO DRINKING WATER?
According to the American Dental Association (ADA), American Academy of Pediatric Dentistry (AAPD) and Center for Disease Control (CDC) water fluoridation is the single most effective public health measure to prevent tooth decay. In the early 1930s, scientists found that people who were brought up in areas with naturally fluoridated water had up to two-thirds fewer cavities compared to those who lived in areas where the water was not fluoridated. Today, several studies show that water fluoridation reduces tooth decay by 20-40%, even with exposure to other fluoride-containing products, such as fluoride toothpaste.
If you suspect the water you consume has lower than optimum concentration of fluoride, for example, if you use well water, filters that remove fluoride, or only use non-fluoridated bottled water, fluoride supplementation may be indicated. Fluoride supplements can be prescribed for at-risk children as drops, lozenges or tablets, with the dose varying with the level of fluoride contained in your water supply and age of the child. The use of fluoride supplements by pregnant women does not result in any benefit for the baby.
WHAT DOES FLUORIDE DO?
Fluoride is said to protect the teeth in two ways:
- Protection from demineralization - when bacteria in the mouth combine with sugars they produce acid. This acid can erode tooth enamel and damage our teeth. Fluoride can protect teeth from demineralization that is caused by the acid.
- Remineralization - if there is already some damage to teeth caused by acid, fluoride accumulates in the demineralized areas and begins strengthening the enamel, a process called remineralization.
According to the National Health Service, fluoride disrupts the process of tooth decay by:
- altering the structure of the developing enamel so that it is more resistant to acid attack. These structural changes occur as a child's enamel develops (before he/she is seven years old).
- providing an environment where better quality enamel is formed, which is much more resistant to acid attack
- reducing the bacteria's (bacteria in plaque) ability to produce acid, a major cause of tooth decay
WHO NEEDS FLUORIDE?
Almost all public health authorities and medical associations agree that children and adults both can benefit from fluoride. Systemic Fluoride, which is the fluoride in water and foods, and is ingested, helps in proper development of teeth that are not yet erupted. Topical fluoride, on the other hand, is the fluoride in tooth paste and fluoride applied to teeth by a dental professional. Topical fluoride affects the teeth that are already in the mouth. For children, AAPD (American Academy of Pediatric Dentistry) recommends in-office fluoride application 2-4 times per year, frequency determined based on each child's caries risk assessment.
Several people, especially those at higher risk of tooth decay, benefit from fluoride treatment. This includes individuals who have:
- A history of tooth decay (cavities)
- Inadequate oral hygiene
- Diets that are high in sugars/carbohydrates
- Snacking habits
- Bridges, crowns, braces, and appliances
- Special needs individuals
- Patients who are on certain medications which affect the oral conditions/flora
- Certain systemic conditions that directly or indirectly affect the mouth, i.e., acid reflux
- Patients born prematurely with dental and/or medical implications
- Individuals with eating disorder
- Enamel defect
- Defective restorations
- exposed roots
- Familial high caries rate
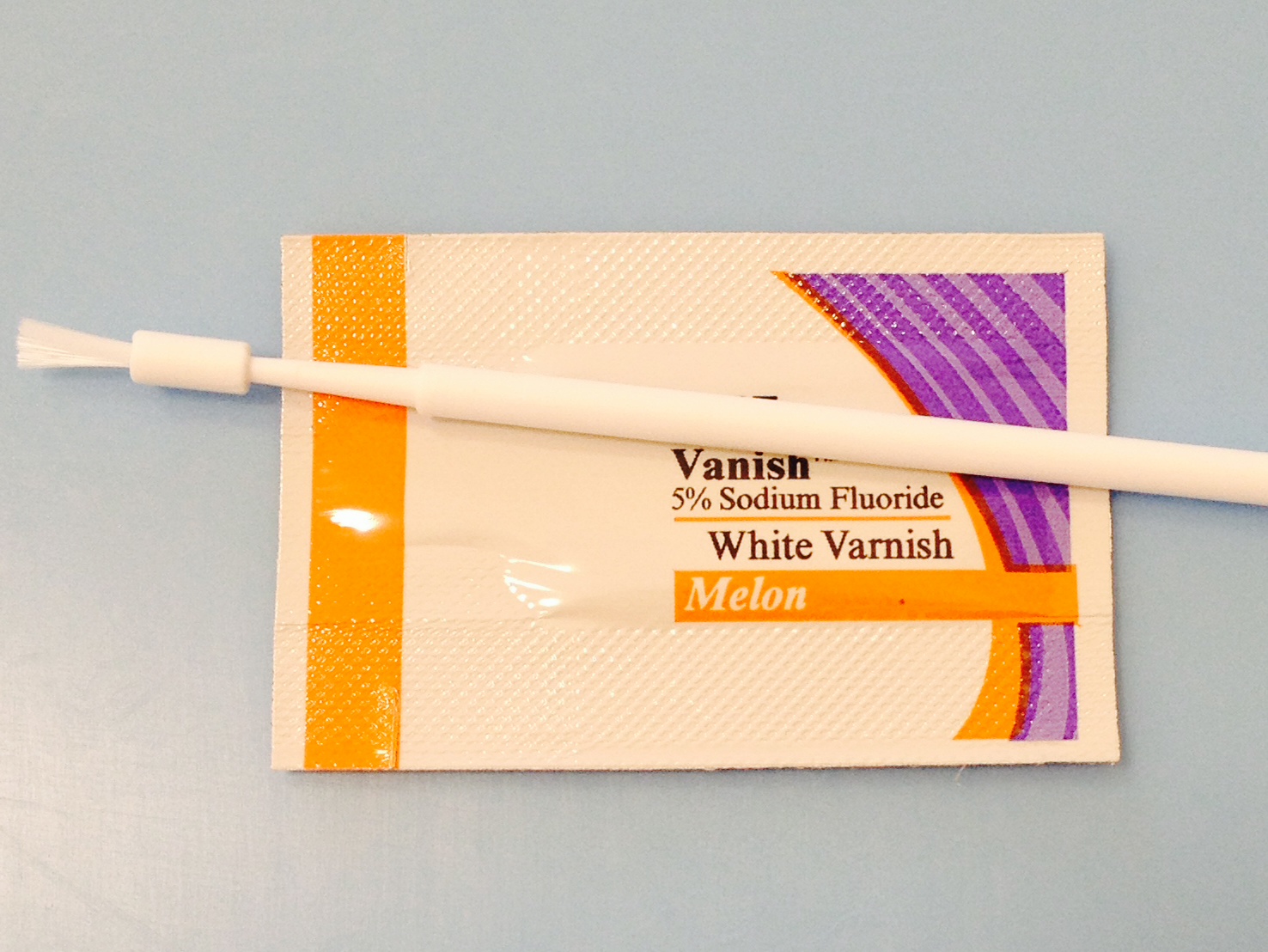
One example of fluoride varnish with its applicator.
In-office Topical Fluorides
In-office fluorides are available as varnishes, gels, foams, and rinses. They differ by type of fluoride, concentration, and method and length of application. The selection, use and frequency of use is based on individual patient's caries risk level, assessed by your pediatric dentist who will be able to discuss your child's caries risk level, ADA and AAPD recommendations, product efficacy, clinical support and safety, ease of use and patient preference/tolerance for maximum results. Fluoride varnishes are becoming more and more popular not only in dental offices but also in pediatric and general medical practices. Varnishes contain higher fluoride level than other forms of in-office fluorides. It is of great importance to evaluate all factors involved before applying varnishes to ensure best results attained from the procedure, but most importantly to minimize ingestion which may contribute to fluorosis of permanent teeth amongst other health issues. These factors are determined through a complete history taking and a thorough evaluation of your child's teeth, diet and home dental care routine. Once fluoride treatment is indicated by your dentist, a trained personnel can apply the varnish, using dosage guidelines and proper technique.
SEALANTS: IT'S PREVENTIVE DENTISTRY
WHAT ARE SEALANTS?
A dental sealant is a flowable plastic coating (clear or white) that flows into the pits and grooves of teeth, and when cured hardens and "seals out" food particles, plaque and bacteria from these high risk areas.
It's been estimated that 90% of tooth decay in school children occurs in pits and fissures. (Kaste 1996)
At Tooth & Co Pediatric Dentistry we apply sealant material that is white (easily detected), BPA and BPB free.
why sealants are indicated?
Even if your child brushes his or her teeth regularly and carefully it is very difficult, and sometimes impossible, to clean in the very tiny pits and grooves present in some of the molars. Some grooves run deep and are a perfect hiding place for plaque and decay-causing bacteria (figures 1 & 2, courtesy of dentalcare.com). In many instances, decay starting at the base of a deep grove goes un-noticed until it is big enough to be diagnosed visually and/or on the x-ray. By then the child may be experiencing toothache and/or need a more invasive and expensive procedure, such as a filling, or pulp treatment and a crown. Tooth decay occurs much faster in children than in adults.

Fig 1. Note the irregularities in this typical permanent molar.

Fig 2. A longitudinal section of a fissure.
Sealant flows into the crevices of teeth and "seals out" plaque and bacteria. By creating a smoother surface in the chewing surfaces of the molars your child can even brush out the sticky foods more effectively (Fig 3 & 4).
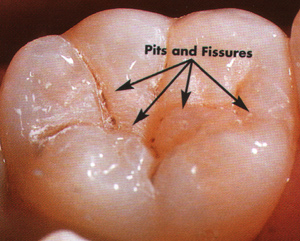
Fig 3. Normal anatomy of a lower molar before sealant.

Fig 4. The molar above with sealant in place.
HOW ARE SEALANTS APPLIED?
Application of sealants is a pain-free and quick procedure that is often performed during your child's routine exam and cleaning appointment. It is also a procedure for which most insurances provide coverage, however, we can assist you in finding out more details on your particular plan benefits.
The tooth, often a molar or a premolar, is cleaned, conditioned and dried.
Sealant is applied with a tiny brush and allowed to flow into the irregularities of the tooth.
A special light is used to cure the sealant in a matter of seconds.
The entire procedure takes a minute or two for each tooth. Your child will be able to eat and drink as normal immediately after the appointment. For sealants to last for years, the integrity of margins of sealants is checked at your child's routine dental visits. Due to normal everyday functions, such as brushing and chewing foods, sealants may be dislodged or damaged. In such instances, new sealant may be applied to repair or replace the original sealant.
"When a child receives sealants, they are 5.22 times less likely to experience caries on all surfaces than children that do not receive sealants. (Bravo and colleagues) Ongoing research continues to find this procedure effective, safe, and of a low enough cost that all populations can access this service. With the use of fluorides, regular dental evaluations, patient education, plaque control, reduction of sugar exposure, and the use of dental sealants, successive generations will have healthy, non-restored dentitions." ( Mary Ann Haisch, RDH, MPA)

DENTAL HOME
According to the American Academy of Pediatric Dentistry the dental home is the ongoing relationship between the dentist and the patient, inclusive of all aspects of oral health care delivered in a comprehensive, continuously accessible, coordinated, and family-centered way. Establishment of a dental home begins no later than 12 months of age and includes referral to dental specialists when appropriate.
At Tooth & Co Pediatric Dentistry, we want to make it easy for expecting parents and parents with infants up to one year of age by offering a complementary visit. Come see our office, meet our staff, and be ready to raise a cavity-free generation.
PREVENTIVE DENTISTRY
PREVENTIVE DENTISTRY specifically against dental caries (which is the disease that leads to tooth decay) starts with understanding the culprits. In order for dental caries to develop, four interrelated factors must occur:
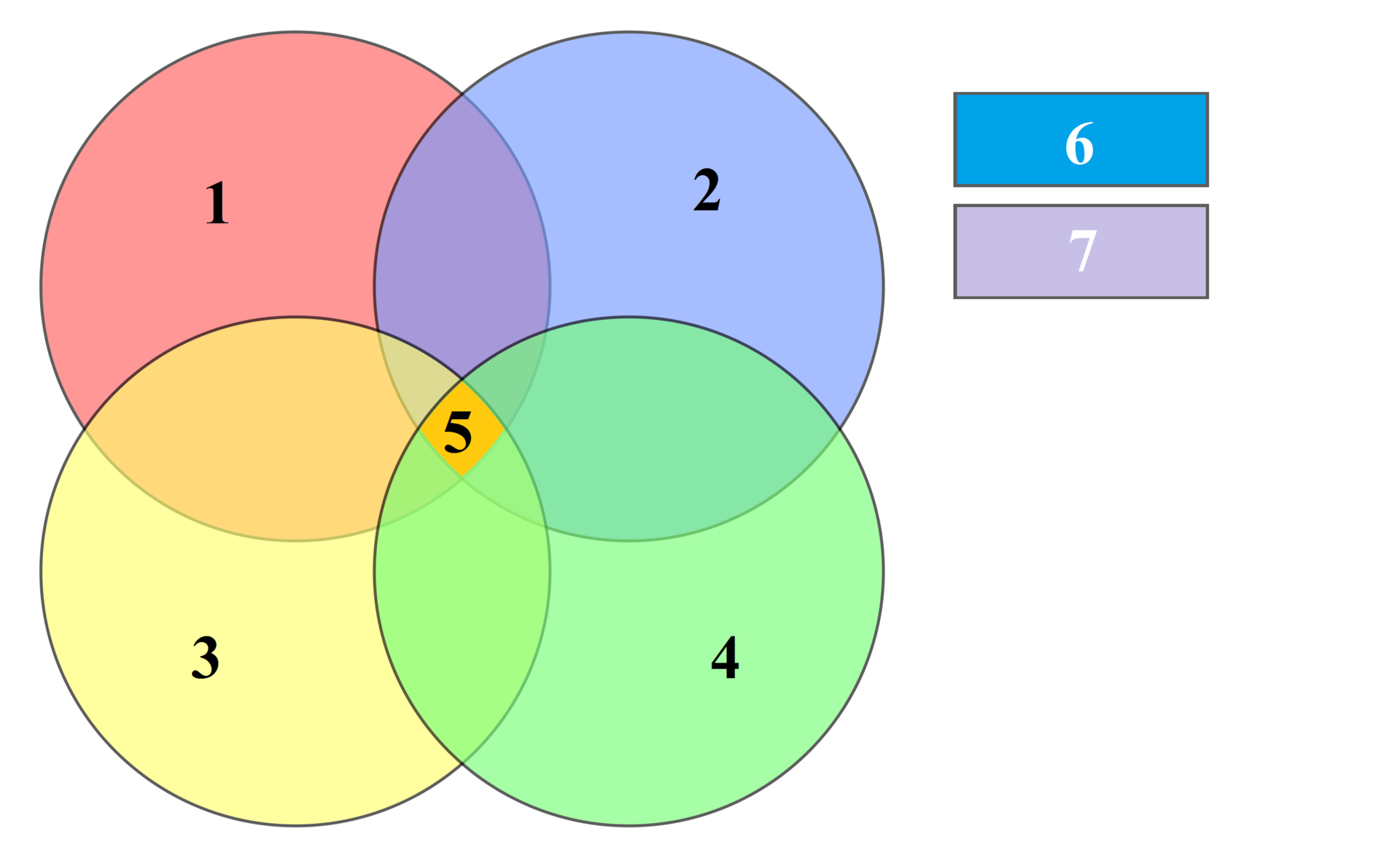
(1) A suitable carbohydrate substrate,
(2) bacteria present in plaque,
(3) a susceptible tooth surface,
(4) time
(5) caries
(6) saliva and (7) fluoride are modifying factors.
There are 3 levels of preventive dentistry:
PREVENTION Step One is to prevent the transmission of the caries causing bacteria (Streptococcus mutans = 'sugar bugs') and delay their establishment in infants, toddlers, and young children. Studies show that these bacteria are transmitted vertically, from the child's primary caregiver(s), AND horizontally, from other family members, such as siblings, and peers. The higher the count of bacteria present in the caregiver's mouth, the more risk for the child. Also, the earlier the bacteria are introduced into the child's mouth and the greater number of bacteria present, the more likely it is that caries will develop in both primary (baby teeth) and permanent dentition. The "window of infectivity" of S. mutans is usually between ages 19 months and 31 months. For these reasons, education of the parents and other caregivers is extremely important and constitutes a major part of your child's first dental visit, at no later than one year of age.
PREVENTION Step Two prevents, arrests, or reverses the microbial shift before any clinical signs of the disease, caries, occur. Now, the caries causing bacteria are established in the mouth. In those areas where plaque accumulates and is often missed during home care, the bacteria count is higher. These areas are generally the pits and fissures in the back teeth, between teeth that are in close contact and at the gum-line of almost all dentition. Removal of dental plaque, whether daily at home or professionally at the office prevents and arrests demineralization (loss of calcium and phosphate) of the underneath enamel, and fluoride application arrests and even reverses the susceptibility of enamel to decay. During your child's dental visit, your pediatric dental team will evaluate your child's oral hygiene, assess their individual caries risk, and provide education on effective plaque removal. Newly erupted teeth are more porous and go through a post-eruption secondary maturation, during which enamel becomes fluoridated and more acid-resistant. Infants, especially, benefit from in-office fluoride varnish application since their teeth have limited exposure to fluoride, another reason why first dental visit by first birthday is a major part of prevention.
PREVENTION Step Three focuses on limiting or stopping the progression of the caries process by initiating remineralization therapy of existing lesions. Demineralization, or loss of minerals calcium and phosphate, occurs when the saliva pH drops from a neutral level of 7 to an acidic level of 5 and lower. Acid conditions come about when refined carbohydrates are introduced into the oral cavity, S.mutans ('sugar bugs') present in the mouth consume the carbohydrates and produce lactic acid. Common reasons for prolonged acid conditions include: increased carbohydrate intake, reduced clearance of lactic acid due to low saliva content, biofilm/plaque accumulation due to insufficient oral hygiene care, and presence of teeth with cavities. The more 'sugar bugs' present, the more acid produced, the more demineralization.
Remineralization, or regaining of minerals, occurs when saliva is released in the oral cavity returning the pH to the neutral level of 7. It is also important that minerals calcium, phosphate and fluoride are locally available to enamel for uptake. The balance between demineralization and remineralization is crucial. If demineralization occurs too frequently, then an incipient lesion (also referred to as a 'white spot' or 'start of a cavity') will occur. Incipient lesions may take up to 9 months or more to be seen and diagnosed in an x-ray. Early establishment of a dental home, followed by routine dental visits (frequency determined through customized caries risk assessment), will ensure early detection and treatment of incipient lesions, thus preventing cavities.
For more information on preventive dentistry visit aapd.org or ada.org.